

The Most Important Test You’ve Never Heard Of
In May 2020, Stanford scientists developed a test that could have altered the course of the pandemic response. It was never rolled out.


In spring 2020 the public was bombarded with a message that would soon permanently embed itself into the national consciousness: people without Covid symptoms could unknowingly be infected and—more importantly—transmit the virus to others. This was the justification given by Anthony Fauci in the first week of April 2020 for his 180 on community mask recommendations. “A lot of people who were asymptomatic” were spreading infection, he said, so everyone should wear a mask. A chorus of public health professionals, including Scott Gottlieb, the former commissioner of the FDA, made the same argument. As did the CDC.
The specter of asymptomatic transmission undergirded not just policies on masks, but on distancing, and quarantines as well. The concept of “silent spread” was so influential that Deborah Birx, the White House Coronavirus Response Coordinator, named her book Silent Invasion after it. The entire apparatus of our pandemic response—which, most consequentially, kept millions of healthy children out of full-time school for more than a year—was based on this notion.
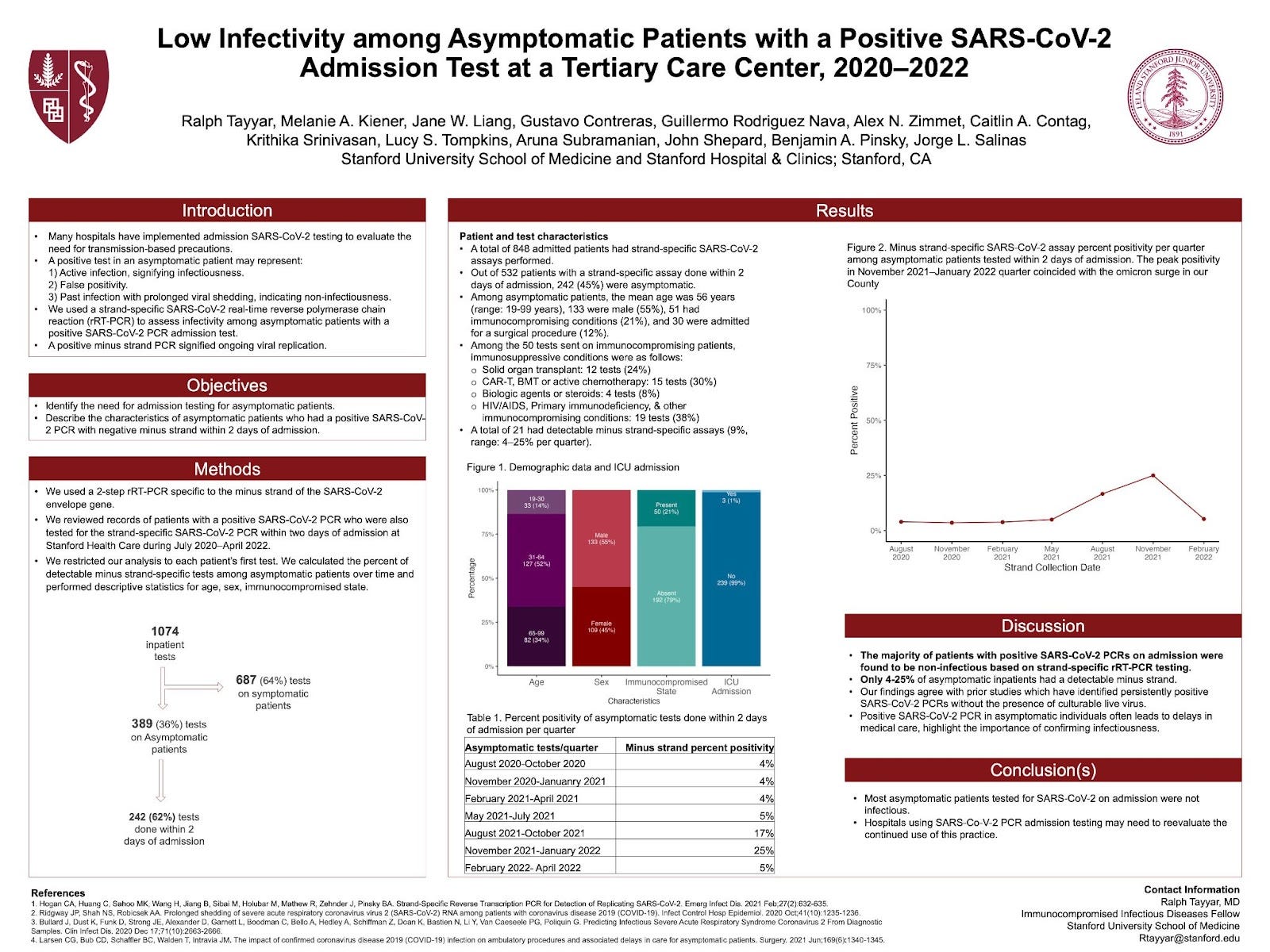
Now, a paper from researchers at Stanford University School of Medicine and Stanford Hospitals, raises an extraordinary prospect: transmission from asymptomatic people is far, far less common than we were led to believe.
From a special test they developed, the researchers found a remarkable 96 percent of people who were PCR-positive but without symptoms were not infectious.
Most people who don’t have symptoms, of course, are not infected. So the likelihood of someone who is not noticeably sick actually being infected and infectious was exceedingly rare. This means that much of the actions we were told—or compelled—to take, including an acceptance of all those closed or half-empty schools, had little to no benefit.
Worse still, the novel test at Stanford that showed a very low rate of infectious asymptomatic people who had tested positive was available as early as May 2020. Yet the CDC and other health authorities did nothing.
***
Despite the narrative, the idea that substantial portions of infections were acquired from people without symptoms never had a strong evidence base. In June 2020, Dr. Maria Van Kerkhove, head of the World Health Organization’s emerging diseases and zoonosis unit, said that transmission from asymptomatic people was “very rare.” This conclusion was based on a number of countries doing very detailed contact tracing, she said. (The next day, after criticism from some health professionals, WHO officials walked back her statement, and Van Kerkhove said it was a “complex question.”)
Authors of an editorial reviewing the evidence of asymptomatic transmission, published in BMJ in December 2020, said “Searching for people who are asymptomatic yet infectious is like searching for needles that appear and reappear transiently in haystacks.”
Some views went in the other direction. The following month, a paper in JAMA Network Open suggested that more than half of all transmission came from infected people without symptoms. Naturally, this finding—which supported the health authorities’ messaging, and justified various community interventions—was covered everywhere, from CNN to PBS to NBC to FOX. Yet this conclusion was based on mathematical models, which are based on numerous assumptions and subjective choices by the researchers; which is to say, in layman’s terms, it’s a guesstimate.
Other than models, evidence of a higher proportion of transmission being from infected people without symptoms was based on epidemiological studies, which typically were of a particular cluster or outbreak, not of large population groups, making extrapolations difficult.
In short, plenty of studies have demonstrated that, indeed, people without symptoms can transmit to others. That’s never been a mystery. It’s also long been known that people without symptoms can transmit other respiratory viruses, such as influenza. SARS-CoV-2 also having that capability should not have been presented as revelatory.
The question has never been can people without symptoms transmit SARS-CoV-2, but rather to what extent this occurs in the general population.
The Stanford test does not answer that question specifically, but it tells us something related that’s more important: how likely is it for someone who has Covid but doesn’t have symptoms to be infectious?
***
Most everyone has heard of the standard PCR test, which detects whether someone has the virus. But it cannot detect whether the person is capable of infecting others. In May 2020, the Stanford researchers created a specific PCR test that could do this. Here’s how:
PCR tests work by using a process called cycle thresholds, where the viral RNA is amplified over and over until it’s detectable. The higher the Ct, the less virus that is present, so the number of cycles can provide a rough approximation of infectiousness, but it’s still just an educated guess. If the Ct is too high the person is shown to be “positive” but the test merely detected fragments of noninfectious genetic material, like a piece of hair left at a crime scene.
SARS-CoV-2 is a positive or “plus-stranded” RNA virus. For it to replicate it must do so with a minus strand. Brilliantly, the Stanford test looks to see if the minus strand is present. If it is then that indicates the virus is actively replicating, which means it’s potentially infectious. If the minus strand is absent then the virus is not replicating. (It is not possible to transmit the virus if it is not replicating.)
The purpose of the test, Dr. Benjamin Pinsky, one of the authors of the original paper on the test, explained, was to help clinicians in the hospital accurately find out if patients were infectious or not. Hospitals were delaying procedures and delaying treatments such as chemotherapy, and implementing various infection control measures unnecessarily on patients who tested positive on a regular PCR but who were not infectious. The minus strand test gave a definitive answer one way or the other.
The only other way to know for sure if the virus is replicating is to culture it. But that procedure requires stringent biosafety precautions in special laboratories, a circumstance that is not commonplace. The minus strand test, on the other hand, could be adapted for routine clinical laboratory testing.
To be clear about the importance of all this: as early as May and June of 2020, a test existed that, if it had been rolled out in medical centers and regular labs nationwide, could have enabled people to know for certain whether they were infectious or not. Unlike the ambiguities of epidemiological studies or models, this was a biological test. The CDC ultimately published Pinsky and his colleagues’ paper about the test in January 2021, but it began use at Stanford more than seven months earlier.
This raises serious questions for those in charge of the CDC, NIH, and NIAID for why resources were not allocated toward making this test broadly available.
Though the test was developed for use in hospitals, its utility outside of a medical setting is obvious. Regular people could have paid for the test to find out after they got over a bout of Covid whether they were still infectious or not, enabling them to go to work, visit relatives, and so on. Millions of kids could have tested out of isolation.
More broadly, the CDC could have immediately conducted a huge study to actually answer the question health officials had only been conjecturing about—what percent of positive people without symptoms have the capability of infecting others.
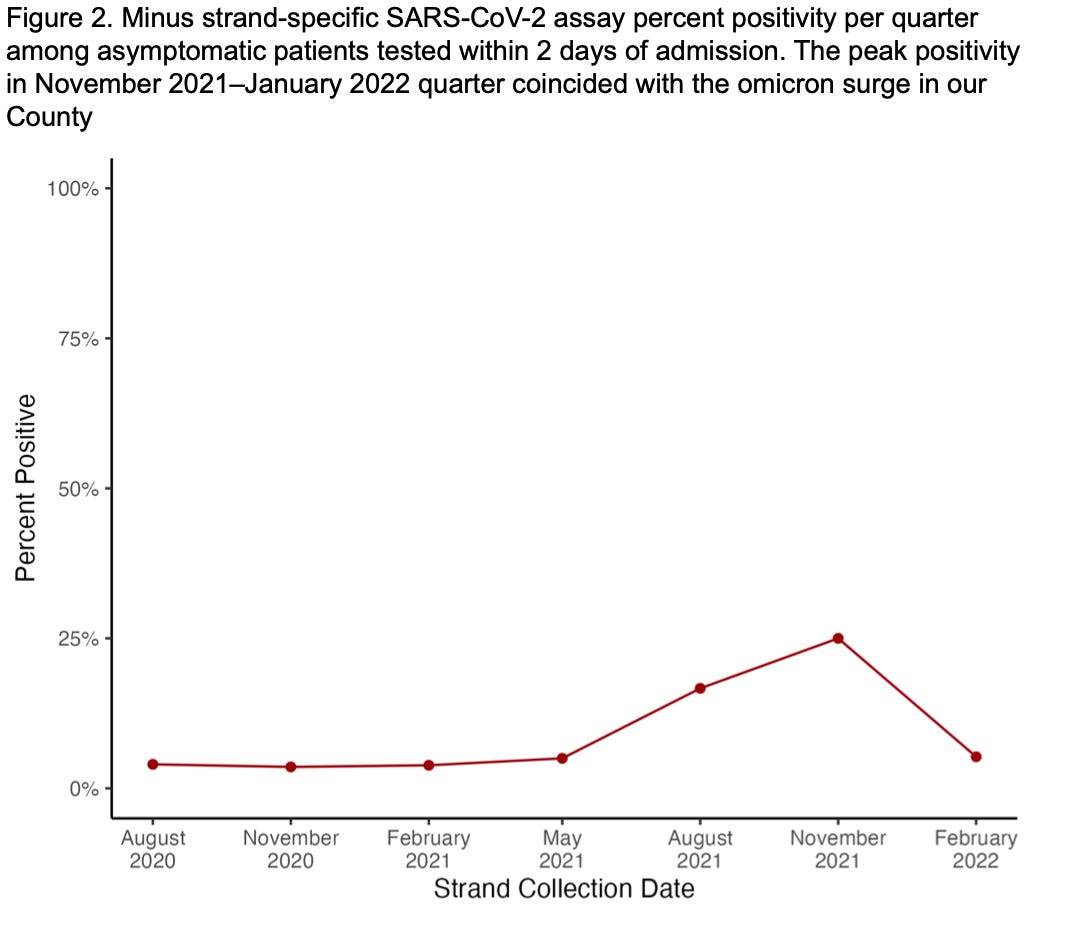
Enter the second groundbreaking piece to this story. Researchers at Stanford later looked at data from this test from July of 2020 through April 2022 and answered the question health authorities neglected to answer. And what they found does not match the narrative about a common threat of people walking around without symptoms infecting others. For the majority of the pandemic only 4% of asymptomatic SARS-CoV-2 PCR-positive patients were shown to be infectious. (During the Omicron wave, the percentage peaked at about 25%.)

I spoke with Dr. Ralph Tayyar, an infectious diseases fellow at Stanford, and an author on the second paper, which is not yet published but was presented at the Society for Healthcare Epidemiology of America’s annual conference last month. He agreed that the effect of imposing nonpharmaceutical interventions on non symptomatic people was probably lower than what we were told.
“The probability of a kid in class who is not sick actually being infectious is very low,” he said. Think about it this way: even if every single student in a school without symptoms was infected, 96 percent of them still weren’t capable of transmitting to others. Yet, of course, most people without symptoms are not infected. Moreover, just because 4 percent were technically capable of infecting others does not mean that in actuality they had sufficient amount of replicating virus to do so. We are talking about a subgroup of a subgroup of a subgroup.
On this point, in relation to hospitals, Tayyar told me that after their study Stanford stopped doing admission screen testing. There is no evidence this led to an increase in transmission versus hospitals that continued testing all new admissions.
I spoke with two other infectious diseases physicians, both at major university hospitals, who spoke on the condition of anonymity because they were not authorized by their institutions to talk publicly about the test and study. “All of that data on PCRs had a huge influence on policy decisions. And influenced people’s fear and anxiety of asymptomatic spread,” one of them told me.
When I discussed the Stanford papers with him, Dr. Daniel Morgan, a physician and professor of epidemiology and public health at the University of Maryland School of Medicine, said “the vast majority of positive PCR Covid tests in asymptomatic patients did not detect patients who were infectious.” He added, “During the pandemic we focused too much on testing, using tests with known issues, and too little on risk based approaches. We took a zero tolerance approach assuming that covid transmission would be impacted and that it was the only goal of public health policy.”
This doesn’t mean nothing should have been done. As Dr. Pinsky of Stanford told me, “All biomarkers of infectivity, including the minus-strand test, should be interpreted cautiously in clinical practice.” And when I discussed the Stanford test and the resultant papers with Louise-Ann McNutt, an infectious diseases epidemiologist at SUNY Albany, she said, “before I would make policy at hospitals or schools more data is needed.”
But it is clear that the harms of overstating the prevalence of asymptomatic transmission were real. Asymptomatic COVID testing added 1.89 hours to the length of stay in the emergency department of an academic health system, and a study found it cost more than $12,500 to identify one asymptomatic COVID patient.
Outside of hospitals the harms were arguably far more extensive. Schools, if they were open at all, operated at half capacity in order to comply with distancing rules; in many states all children were required to mask all of the time; and students were quarantined repeatedly for long stretches of time, even though they were not infectious—all of these rules, that kept healthy children home or in masks, were based on the idea that we didn’t know who could be infected and contagious.
We were made to believe that each of us was a potential, unwitting one-person-WMD. Who can forget those video illustrations all over social media and major news outlets of little, red poison dots floating out of people’s mouths and noses toward innocent individuals nearby? While medical centers and other places with particularly vulnerable people may have benefited for some time from the more stringent rules, schools—as they did in Sweden—and most of society could have simply followed the classic advice “if you’re sick, stay home,” and we would have ended up in the same place.
I have been following Carl Heneghan since the start of this debacle and he was very much screaming about the misuse of PCR tests as they did not give information on infectivity. I sent his original piece on this topic to my family members in California and received little interest. Thank you for another great piece.
It also shows once more how emergencies - alleged or real - are the worst moments to stifle debate or to censor dissident voices.